
Spike Mitigation, Spike Retention, and Spike Antibodies
Neo7 Personalized Peptide Spike Mitigation Corrects Corrupted Protein Signals and Restores Health


Presented By: Neo7Bioscience and the McCullough Foundation
Spike Mitigation, Spike Retention, and Spike Antibodies
Neo7 Personalized Peptide Spike Mitigation Corrects Corrupted Protein Signals and Restores Health
Across the globe, millions of individuals are now living with persistent mRNA-derived spike retention and multisystem biological disruption, presenting with patterns of illness that modern medicine struggles to explain using conventional immune or organ-specific models. This is not a marginal phenomenon or an anecdotal signal. It is a worldwide molecular pathology unfolding in real time.
Patients report alarming, heterogeneous, and often devastating symptoms spanning nearly every physiological system, including:
Severe brain fog, cognitive slowing, memory loss, executive dysfunction, and neurobehavioral changes
Myocardial and pericardial inflammation, conduction abnormalities, dysrhythmias, autonomic instability, and unexplained exercise intolerance
Kidney, lung, and skin disturbances, frequently without correlating structural findings on routine imaging
Biome and microbiome disruption, gastrointestinal instability, immune–metabolic imbalance, and loss of mucosal resilience
Progressive systemic fibrosis and tissue destruction, affecting vascular, connective, and parenchymal compartments
Marked elevation in oncogenic signaling, increasing risk for cancers of every type—often emerging without predictable tissue specificity, latency, or prior risk stratification
What unites these presentations is not a shared diagnosis or antibody pattern, but a shared molecular signature: transcriptional instability, corrupted protein signaling, and persistent intracellular stress driven by spike-related interference.
This brings medicine to a necessary reckoning:
Neutralizing an antigen is not the same as repairing the molecular damage it leaves behind.
This distinction defines the work of Neo7Bioscience.
Neo7 does not chase symptoms.
Neo7 does not chase antibody titers.
Neo7 corrects spike-induced signaling dysfunction at its molecular root.
Spike Pathology Is Not Binary—It Is Systemic and Persistent
Conventional frameworks treat spike biology as binary: present or absent, neutralized or cleared. Patient molecular data tell a far more complex story. Spike exposure can induce:
Persistent receptor-binding domain (RBD) interactions
RNA transcriptional volatility across immune, metabolic, and stress pathways
Protein misfolding and impaired intracellular clearance
Endothelial, mitochondrial, and neuroinflammatory signaling instability
Oncogenic, fibrotic, and maladaptive repair programs
These abnormalities frequently persist independently of viral clearance and often coexist with robust antibody levels. In such cases, the immune system has recognized spike—but the biology has not recovered.
The Neo7 Strategic Hub: From Molecular Surveillance to Molecular Correction
Neo7 was built as a strategic precision-medicine hub to address this exact failure point in modern care. Its platform integrates:
Longitudinal molecular surveillance
RNA expression and pathway activity are measured directly in each patient—never inferred.Signal prioritization
Spike-related dysregulation is mapped across immune regulation, mitochondrial function, endothelial integrity, transcriptional control, and repair systems.Personalized peptide engineering
Peptides are designed to correct only the pathways demonstrably distorted in that individual’s molecular data.
This is not population-based treatment.
It is an expression-driven biological correction.
Designing Spike-Mitigation Peptides at the RBD and Transcriptional Level
Neo7 molecular scientists engineer spike-mitigation peptide sequences with a precise objective:
Interrupt spike-driven transcriptional instability at its molecular origin.
Design begins at the receptor-binding domains (RBDs)—not simply to block interaction, but to neutralize the downstream signaling chaos those interactions induce. Peptides are constructed to:
Bind RBD-associated pathological motifs
Silence spike-induced transcriptional volatility
Normalize downstream immune, metabolic, and stress signaling
Support endogenous repair without immune overstimulation
This is not antibody mimicry.
It is a signal correction.
Beyond Spike: Examples of Additional Correction Motifs
While spike proteins often initiate the molecular insult, they are rarely the sole drivers of ongoing pathology. Neo7’s surveillance repeatedly shows a secondary network of dysregulated host pathways that continue to propagate disease even after spike signaling itself is mitigated.
Accordingly, peptide engineering extends to adjacent and downstream correction motifs—targets reflecting how the patient’s biology has been reprogrammed by exposure. Depending on RNA expression, sequences may be designed to normalize:
Innate immune regulators (interferon programs, NF-κB modulators, inflammasome transcripts)
Mitochondrial bioenergetics (oxidative phosphorylation, mitophagy, redox balance)
Endothelial and vascular signaling (coagulation imbalance, nitric oxide pathways, microvascular inflammation)
Protein quality control (autophagy, unfolded protein response, proteostasis)
Fibrotic and oncogenic transcription (TGF-β-linked fibrosis, aberrant growth signaling, DNA repair imbalance)
Neuroimmune and autonomic control (glial activation, neuroinflammatory, and autonomic imbalance)
Each target represents not a diagnosis, but a measurable deviation from healthy transcriptional order.
Correction Motifs Are Chosen by Expression—Not Assumption
Targets are never preselected by diagnosis alone. They are chosen because the patient’s molecular data shows they are:
Abnormally upregulated or suppressed
Functionally linked to symptoms
Mechanistically connected to spike-induced transcriptional volatility
The resulting peptide sequences act as precision correction motifs, guiding cellular systems back toward coherent signaling rather than forcing broad immune activation or suppression.
Antibodies Do Not Equal Recovery—and Cross-Reactivity Confounds Interpretation
A central misconception in post-spike medicine is that antibody decline reflects healing. In reality, antibody levels may never fall, and their persistence often bears no correlation with clinical improvement.
This is further complicated by antibody cross-reactivity. Spike antibodies can bind conserved or host-adjacent epitopes, generating immune noise that obscures true biological status. Persistently elevated antibodies may reflect immune memory decoupled from pathology, epitope overlap, or ongoing recognition without active damage.
Antibodies measure exposure.
They do not measure recovery.
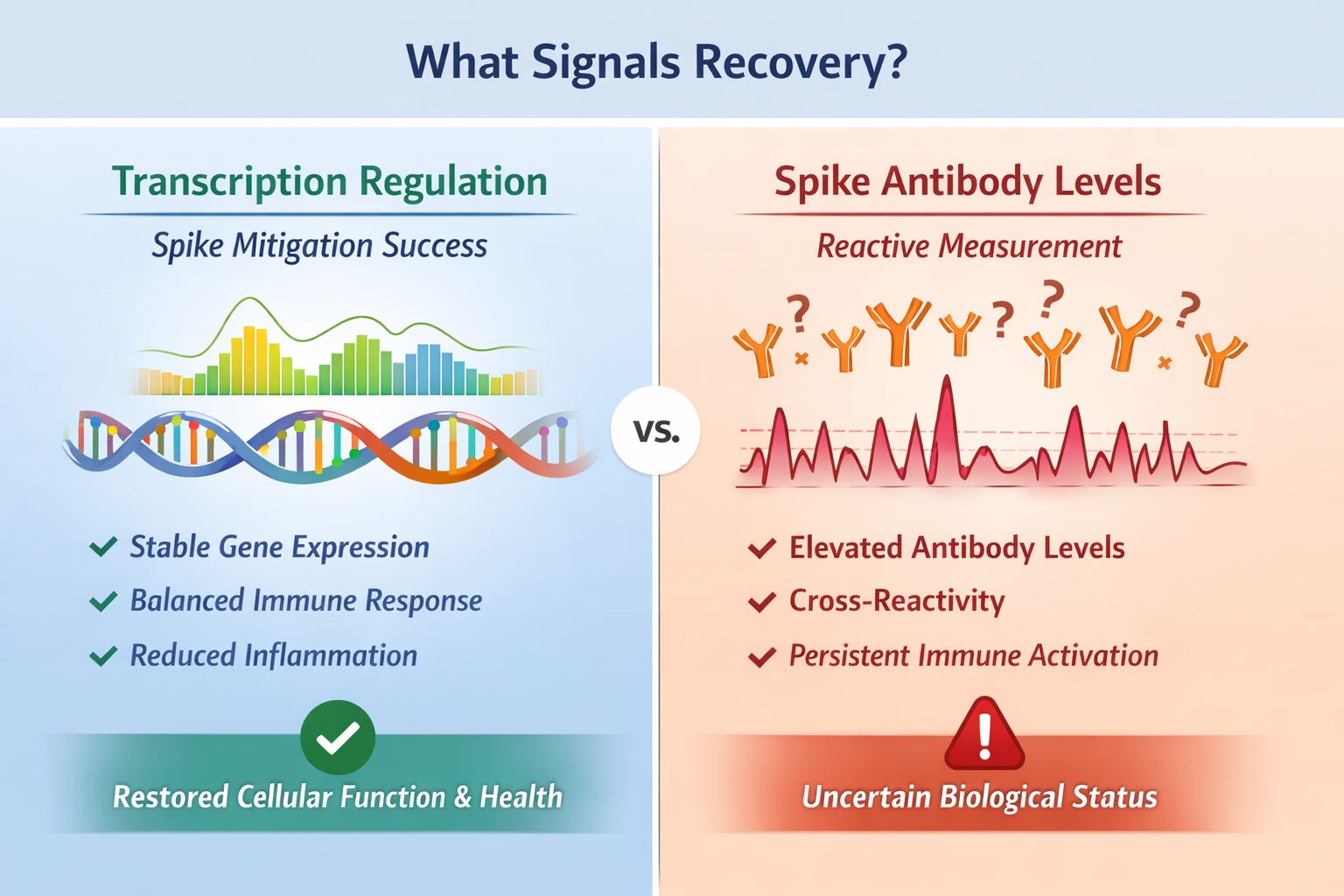
RNA Transcription Markers Are the True Indicators of Healing
Across Neo7 surveillance, meaningful recovery correlates with normalization of RNA transcription markers, not antibody titers. Improvement aligns with:
Resolution of aberrant interferon and inflammatory programs
Stabilization of mitochondrial and metabolic transcripts
Correction of endothelial and coagulation signaling
Downregulation of oncogenic and fibrotic pathways
Restoration of immune regulation rather than immune persistence
These changes often occur while antibodies remain elevated or cross-reactive, because antibodies are downstream artifacts—not the control layer of biology.
RNA transcription governs function.
Antibodies record history.
Multi-Pathway Correction: Addressing the Full Spike Footprint
Spike exposure rarely damages a single pathway. Neo7 peptide systems are designed to correct multiple dysregulated pathways simultaneously, addressing the full biological footprint left behind by spike-induced instability—precisely and adaptively.
Timeline of Response: Weeks to Improvement, Months to Stability
Across patients undergoing Neo7 spike-mitigation and correction-motif protocols, a consistent trajectory is observed:
Within weeks: reduced transcriptional noise, improved signaling coherence, early functional gains
Within ~6 months: stabilized RNA profiles, durable pathway correction, restored adaptive resilience
This reflects true molecular repair, not transient suppression.
Personalized Peptide Administration and Adaptive Re-Assessment
Neo7’s precision peptide programs are designed to remain aligned with dynamic human biology, not static treatment assumptions.
Following molecular surveillance and individualized design, patients undergo:
Intramuscular (IM) administration of personalized peptides twice weekly
A structured treatment duration of approximately six months
Dosing calibrated to promote transcriptional normalization without immune overstimulation
At the end of six months, patients undergo a comprehensive molecular re-evaluation, including RNA transcription markers and pathway-level regulation, to determine:
Which signals have normalized
Which pathways require continuation, modification, or tapering
Whether peptide sequences should be refined, paused, or discontinued
This adaptive loop—measure → correct → re-measure—is foundational to the Neo7 platform.
Recovery is not assumed.
It is measured, verified, and refined.
Beyond Antibodies: Redefining Recovery
Recovery is not the disappearance of antibodies—especially in a landscape complicated by immune persistence and cross-reactivity.
Recovery is the restoration of intelligible molecular signaling.
Neo7’s personalized peptide platform rests on a simple, rigorous premise:
Measure what is broken.
Correct it precisely.
Allow biology to heal.
The critical question is no longer, “Are antibodies still present?”
It is, “Has the molecular signal been repaired?”